














- Welcome
- Lumbar spinal stenosis
Lumbar spinal stenosis
Back
Introduction
Anatomy
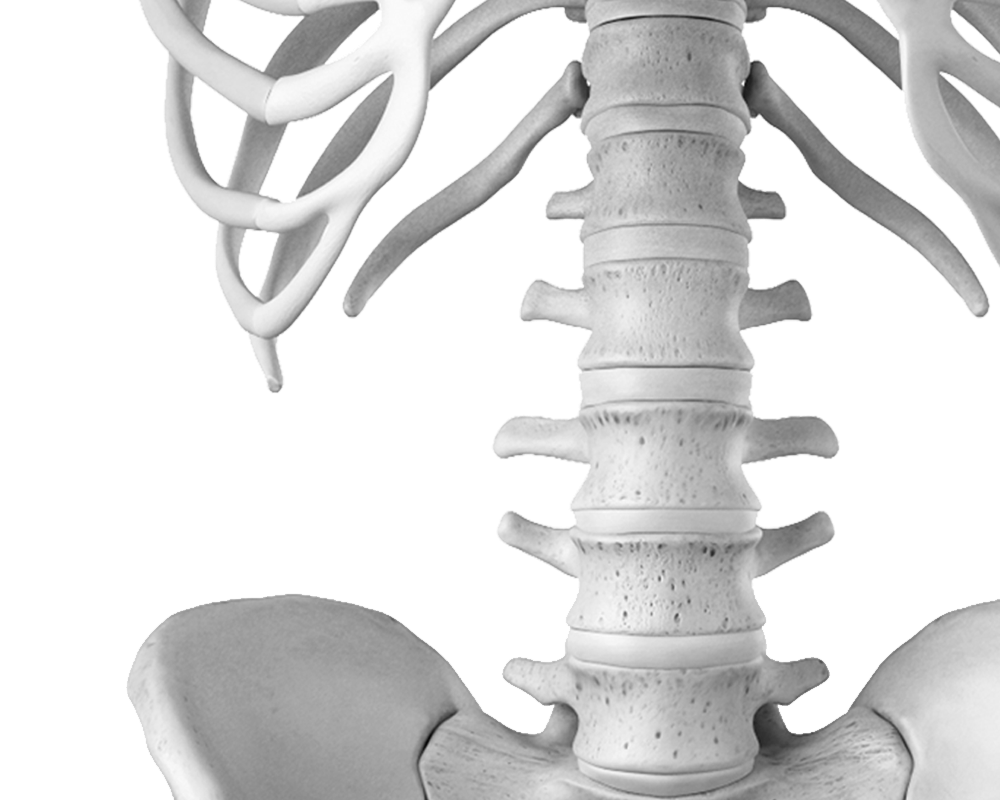
The lumbar spine is the lower part of our back and comprises 5 vertebrae (lumbar vertebrae). These vertebrae consist of a vertebral body at the front and a vertebral arch at the back, which surrounds the spinal canal and nerve structures. Lateral openings (intervertebral foramina) (8) allow nerves to exit the spinal canal to innervate our legs.
The discs are located between the vertebral bodies and act as shock absorbers between the vertebrae. They are formed of a fibrous, elastic, and very strong ring, at the center of which is a ball of gelatinous material (nucleus pulposus). It is thanks to the elasticity of the ring that the nucleus can deform according to the stresses to which it is subjected (body movements, axial or vertical load, resistance against force). The disc and the two vertebrae above and below it form a functional unit called the vertebral segment.
The vertebrae move against each other at the level of the disc anteriorly and at two joints (facet joints) (9) posteriorly. Small movements, on the order of 3 to 5° per segment, are possible in all directions (flexion-extension, lateral flexion on both sides, rotation to the right and left). Considering the entire lumbar spine, the movements are therefore on the order of 15 to 20° in each direction, depending on the patient's age and flexibility. Most of the mobility that we believe occurs in our back actually takes place in our hips.
Signs & symptoms
Patients with spinal stenosis typically complain of leg pain, sometimes radiating to the feet, which is generally aggravated by walking (claudication). This pain is often relieved when the patient sits or bends forward. In most cases, the patient also complains of lower back pain, which can sometimes be quite intense.
In cases of significant nerve compression, pain may be associated with decreased sensation or even weakness in the legs (neurological deficits).
In very rare cases, the patient may experience incontinence (especially urinary incontinence). This constitutes a surgical emergency and the patient must seek immediate medical attention.
What is this?
Sciatica is usually caused by irritation of the nerve as it exits the lumbar spine (nerve roots).
Spinal stenosis is a condition linked to aging, and therefore common from the age of sixty onwards. It was first described only about sixty years ago, probably thanks to improvements in available radiological techniques. It consists of a narrowing of the spinal canal, the tunnel through which nerve structures pass, leading to their progressive compression. The disease involves degenerative changes affecting both the intervertebral discs and the facet joints, resulting in their deformation, thickening of the tissues that compose them, and bony growths.
This condition can affect one or more levels of the lumbar spine, with involvement most often varying degrees of severity. In some cases, spinal stenosis may be associated with segmental instability (increased mobility between two vertebrae) or with lumbar spinal deformity in the form of scoliosis.
Risk factors
- Accidents involving the back, sometimes even of low intensity, especially if they occur repeatedly.
- Some sports activities are too intense, especially if carried out without adequate preparation.
- Repetitive axial (vertical) stresses, performed too intensely (jogging on hard surfaces, ski jumping, lifting weights, etc.)
- Poor back hygiene, especially at work, poor sitting posture. Excess weight. Poor physical condition, and in particular a lack of muscle mass, often linked to age.
- Sedentary professions. Anterior disc surgery. Back fractures.
Screening & Diagnosis
During the medical examination, the anatomical origin of the patient's complaints will be determined, first through a medical history (discussion about the nature of the pain, its onset, what relieves it, and what aggravates it), as well as through a physical examination of the patient, focusing particularly on the lower back and a detailed examination of the legs. A neurological examination may also be necessary at this stage.
The patient will also be able to benefit from radiological examinations including conventional X-rays, a CT scan or, even better nowadays, an MRI examination.
Leg pain similar to that of spinal stenosis can also be caused by poor arterial circulation in the lower limbs. Therefore, tests to rule out arterial obstruction may be necessary as part of the preoperative assessment.
Treatments
Self-treatment
In the absence of neurological deficits (loss of sensation, muscle weakness, urinary incontinence), the patient can begin treatment:
- Reduced physical activity, rest
- Lying down, with a cushion under your knees
- Over-the-counter pain relievers and anti-inflammatory medications
Medical treatments
The presence of lumbar degenerative disorders with disc protrusion or spinal stenosis, which is evident on X-rays or on an MRI, does not in itself represent an indication for surgical treatment unless it can be demonstrated that the cause of the complaints is severe enough to require such treatment.
If possible, a conservative treatment Therefore, non-surgical treatment will always be recommended initially. This will include modifying or even reducing physical activity, pain relievers and anti-inflammatory medications, physiotherapy, and, if necessary, a series of epidural injections.
Surgical treatment will only be considered if the complaints are sufficiently disabling despite conservative treatment followed for a period of 2 to 6 months, or if they are associated with sensory disturbances or muscle weakness in the legs (neurological deficit).
Depending on the patient's complaints, surgical treatment may involve decompression of nerve structures (excision of tissues that reduce the diameter of the spinal canal and compress the nerves), associated or not with fusion of the vertebral segments affected by the pathology.
Our favorite methods
Conservative treatment
As mentioned above, in the absence of neurological deficit (loss of sensation, muscle weakness) we will always start with optimal non-surgical management (rest, medication, specialized physiotherapy).
Epidural or epidural infiltrations
To enhance the anti-inflammatory effect on irritated or compressed nerve structures, an epidural injection can be considered. This procedure is performed under local anesthesia. Under radiological guidance, a needle is inserted until it reaches the nerves (in the epidural space) at their exit from the lumbar spinal canal, where small amounts of cortisone are deposited to maximize their anti-inflammatory effect.
If the complaints improve, the infiltration may be repeated at an interval that the doctor will have to define (3 to 6 weeks).
Facet joint injections
In rare cases where irritation of the nerve structure is caused by advanced lumbar osteoarthritis with the formation of joint cysts, such an infiltration may be offered to the patient.
This procedure is also performed under local anesthesia. Under radiological guidance, the needle is inserted into the affected lumbar facet joint where a few drops of cortisone are deposited.
Surgical treatment
Decompression of nerve structures
If the cause of sciatica is identified as a disc lesion or even a herniated disc, then a microdiscectomy will be performed (see herniated disc).
When the pathology in question is degenerative in severe lumbar osteoarthritis with narrowing of the spinal canal or of the exit window of the nerve root, or even the formation of an articular cyst, decompression of the nerve structures will be proposed (see also "spinal stenosis").
This surgical procedure is performed under general anesthesia through a small incision in your lower back. The incision's location is determined radiologically before the procedure begins. The muscles covering the spine are then separated to allow access to the posterior aspect of the spine. Under the guidance of an operating microscope, the surgeon will open the spinal canal, which carries the nerves. The tissues narrowing the spinal tunnel can then be progressively removed using microsurgical instruments. The patency of the tunnel, allowing passage for the nerves, can be assessed using calibration instruments. The extent of this decompression procedure will, of course, depend on the radiological examinations performed before surgery, which will have allowed for precise planning.
Flexible intervertebral fixation
In some cases, after decompression of the nerves is complete, the surgeon will implant devices to slightly separate the two vertebrae and thus prevent nerve compression from recurring. These separators are generally made of very rigid, non-metallic synthetic materials, allowing for easy postoperative X-rays and MRIs. These devices are placed between the spinous processes of each vertebra and held in place by anchoring straps. The separation between the vertebrae is very slight, on the order of 2 mm, as the implant's primary function is to prevent the two vertebrae from coming together.
Spinal fusion
In rare cases where instability of the vertebral segment has been shown during preoperative radiological examinations, it will be necessary to add to the decompression of the nerves the blocking of the 2 vertebrae concerned (vertebral fusion or spondylodesis).
During these procedures, the two vertebrae are fitted with screws that are inserted using a computer-assisted navigation system, allowing us to position these implants as precisely as possible. These screws are then connected to two rods to create perfect stability between the two vertebrae and to allow the bone graft placed next to the rods to properly fuse (spinal fusion).
These implants are made of titanium, a metal that will allow for future MRI scans if necessary. A small suction drain will be placed at the surgical site before the wound is closed.
After the operation
Upon leaving the operating room (you will be awake), you will spend a few hours in the recovery room. You will be under the care of your anesthesiologist, who will manage your pain. Every effort will be made to ensure your comfort and keep your pain under control. You will be lying on your back, and if you wish, the nursing staff can turn you onto your side. As soon as you are sufficiently awake, the anesthesiologist will authorize your transfer from the recovery room to your room. (see recovery)
Surgery
Preparation for surgery
Lumbar spinal stenosis – Preparation for surgery
We will be in constant communication with your family doctor to discuss and proceed with the best treatment option for you. Once the surgical indication has been established and scheduled, you will receive a summons letter from the Bois-Cerf Clinic containing information regarding:
Pre-hospitalization consultation
Before your hospital stay, you will have a consultation with one of our anesthesiologists to assess your health, perform the necessary tests (blood work, chest X-ray, electrocardiogram), and discuss the anesthesia procedure, which will be general anesthesia. Please be informed of the day and time you should arrive at the reception desk of the Bois-Cerf Clinic (this could be the day before or the day of the procedure).
Hospital stay
What you need to bring with you:
- Your personal belongings
- Reading material if you enjoy reading
- Music player
- Your personal medications (if you are receiving treatment at home)
- Your optimism and energy... we'll take care of the rest.
Upon your arrival at the clinic, after completing the administrative formalities, you will be greeted by the receptionists and shown to your room. The nursing staff will take care of you to ensure you are comfortable. Some tests may still be necessary as requested by your doctors. Skin care (disinfection) will be performed on the area of the future surgical wound.
You will receive visits from your surgeon and the anesthesiologist (pre-operative visits). A physiotherapist will visit to instruct you on breathing exercises and how to move in bed and get up after the procedure. The surgery will generally be performed at the time previously communicated to you by your surgeon.
As in the past, the operation is performed under general anesthesia. Your anesthesiologist will administer premedication one hour before the operation and, if necessary, the evening before, to help you relax and reduce stress related to the procedure. Visitors are generally allowed in the recovery room (approximately one hour after you leave the operating room, one person only) and freely in your hospital room.
Recovery
Whether the procedure consisted solely of nerve decompression or combined with spinal fixation or spondylodesis, the patient will be mobilized and allowed to get up and move around starting the day after surgery, under the supervision of their physiotherapist and nursing staff. In cases of nerve decompression alone, the urinary catheter and surgical drain will be removed the day after surgery. A shower is generally permitted on the second postoperative day.
In cases of spinal fixation, the urinary catheter, surgical drain, and intravenous line will generally remain in place for 48 hours to better manage postoperative pain and allow the patient sufficient time to get up independently and use the toilet. A shower is scheduled for the third or fourth postoperative day.
During hospitalization, physiotherapists will teach the patient rehabilitation exercises and how to properly perform daily living activities. Wearing an elastic lumbar support brace is recommended for 3 weeks (decompression only) and 6 to 8 weeks for spinal stabilization. Hospitalization is usually 4 to 5 days for the first group and 10 to 14 days for the second, depending on the patient's progress and situation at home.
Post-operative pain is relieved during the first few days via an IV line connected to a pain pump that the patient can adjust themselves. Subsequently, pain medication will be prescribed to ensure adequate pain relief, depending on physical activity. The sutures or staples in the surgical wound are removed 10-12 days after the procedure. Upon returning home, you should maintain a quiet lifestyle (you are in recovery). You will need to take care of the surgical wound (according to the instructions you received during your hospital stay).
For the first 3 to 6 weeks depending on the procedure performed, it will be necessary to avoid sitting in very low positions (sofa, armchair), to avoid physical exertion (household chores) and lifting/carrying heavy objects.
Clinical and radiological check-ups are scheduled approximately 6 weeks after the procedure to plan the follow-up care (medication, physiotherapy, return to activity, sick leave, etc.). A physiotherapy rehabilitation program will generally begin after the first clinical check-up (around 6 weeks after surgery, slightly earlier in cases of nerve decompression alone). Physiotherapy focuses on restoring muscle function and strengthening the abdominal muscles, as well as flexibility exercises (neuromeningeal stretching). This program may be conducted on land, sometimes with the assistance of a pool attendant.
The recovery rate depends on each patient and usually requires 4 to 8 weeks off work for decompression alone and 3 to 4 months for combined procedures with spinal fixation.
You will be able to drive a car as soon as you can sit comfortably and without pain, usually 3 weeks after the operation for decompressions and 6 weeks after for spinal stabilizations.
Approximately 90% of patients experience an improvement in their symptoms, or even good relief from their pain and an improvement in their walking distance.
Possible risks
Anesthesia
Since the procedure is performed under general anesthesia, the patient may be exposed to all the risks associated with this technique, especially if their overall health is not optimal (drug allergies, cardiopulmonary, renal, or metabolic problems, etc.). The rate of these complications is low and will be discussed with the anesthesiologist during the pre-hospitalization visit.
Infection
In any operation, there is a risk of developing an infection, a complication which is fortunately rare (at 1%).
Nerve damage
Because the surgeon comes into contact with nerve structures passing through the spinal canal, nerve damage is always possible, even with the use of an operating microscope. According to specialized medical literature, this risk is approximately 11/3T.
The risk of postoperative hematoma formation compressing nerve structures is reduced by the placement of a surgical drain left in place for 24 to 48 hours (less than 1%).
Spinal fixation
In cases requiring spinal fixation, there is a risk that the hardware may come into contact with nerve structures, causing irritation of the nerve roots and consequently postoperative pain (1 to 2 %). This risk is reduced by a computer-assisted navigation system used in the operating room during implant placement.
Failure of bone graft consolidation
In cases requiring spinal instrumentation with bone grafting (spondylodesis), there is a risk of graft resorption and consequently non-union (1 to 5 % according to the specialized literature, figures which depend on the means of fixation used and the number of vertebral segments operated).
Disc prosthesis
The placement of an artificial disc is performed via an anterior approach. Injury to abdominal organs or major blood vessels (aorta, vena cava) may occur during preparation of the anterior aspect of the lumbar spine.
Frequently Asked Questions
How long does the operation take?
Where is the scar?
What is the length of the incision?
Is the operation possible by only numbing the legs (epidural anesthesia)?
When I leave the operating room, will I be lying on my stomach?
How many days will I stay in the clinic?
Will I be in a lot of pain after the operation?
When can I start driving my car again?
What mobility will my back have after spinal fixation?
When can I return to work?
After an epidural injection, when can one resume physical activity?
Should we be concerned about the use of cortisone during epidural infiltration?
Summary
1006 Lausanne
+41215103348
Learn more in videos
Medicol Videos

4:19

1:02:48

1:07:40

17:03

20:32

9:36

29:09

1:41:27

20:36

11:17

11:27

17:37

15:37
Contact one of our specialists on the subject
Ouchy Orthopedic Center
Specialized medical consultations in orthopedics and traumatology in the heart of Lausanne