














- Welcome
- Low back pain
Low back pain
Introduction

Anatomy
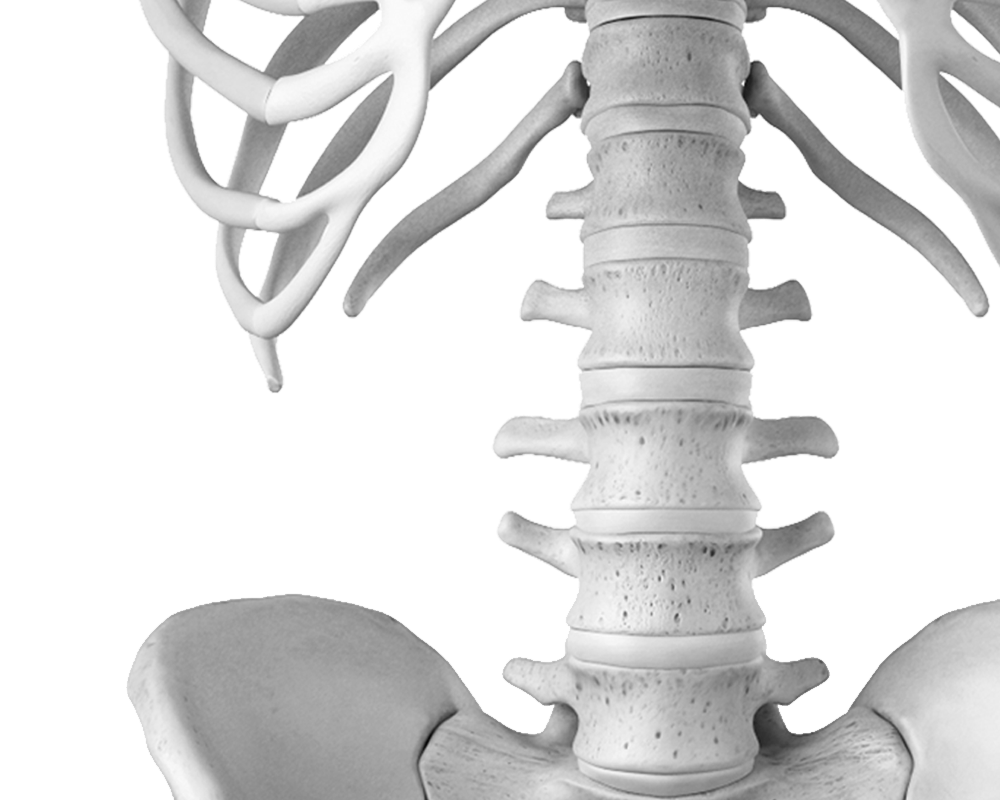
The lumbar spine is the lower part of our back and comprises five lumbar vertebrae. These vertebrae consist of a vertebral body at the front and a vertebral arch at the back, which surrounds the spinal canal and nerve structures. Lateral openings (intervertebral foramina) allow nerves to exit the spinal canal and innervate our legs.
The discs are located between the vertebral bodies and act as shock absorbers between the vertebrae. They are formed of a fibrous, elastic, and very strong ring, at the center of which is a ball of gelatinous material (nucleus pulposus). It is thanks to the elasticity of the ring that the nucleus can deform according to the stresses to which it is subjected (body movements, axial or vertical load, resistance against force). The disc and the two vertebrae above and below it form a functional unit called the vertebral segment.
The vertebrae move against each other at the level of the disc anteriorly and at the level of two joints (facet joints) posteriorly. Small movements, on the order of 3 to 5° per segment, are possible in all directions (flexion-extension, lateral flexion to both sides, rotation to the right and left). Considering the entire lumbar spine, the movements are therefore on the order of 15 to 20° in each direction, depending on the patient's age and flexibility. Most of the mobility we believe occurs in our back actually takes place in our hips.
Signs & symptoms
«Back pain (also called lumbago or lower back pain) is a term used to describe pain primarily in the lower back, which may radiate to a buttock or even the leg. It is important to understand from the outset that not all back or leg pain is the same and can have different causes, even if the symptoms are very similar. Diagnosis and treatment can also vary considerably depending on the nature of the underlying problem.
Lower back pain can be sudden or acute, for example, following a sudden movement, and disappear just as quickly. Back pain can also occur repeatedly or episodically, separated by periods of varying lengths of relief. It can also be chronic, lasting over time and becoming quite debilitating for the patient. Back pain is an extremely common symptom; approximately 80% of the adult population has experienced or will experience an episode of back pain at some point in their lives.
Lower back pain can be constant, present both day and night, or it can occur only during the day, aggravated by certain physical activities such as sitting, walking, standing, or specific movements. In the vast majority of cases, lower back pain is not a particularly serious condition and will disappear after a few days, sometimes even without specific treatment. In other cases, however, it can progress and become increasingly intense, frankly debilitating, and require medical attention.
What is this?
A multitude of diverse causes can underlie back pain or lumbago. It can be caused by injuries to the structures that make up the lower back (discs, joints, joint capsules) or the surrounding tissues (muscles, ligaments, tendons, etc.). It can also be related to aging or the degeneration of all these elements, as occurs throughout our musculoskeletal system. Vertebral fractures, resulting from an accident or related to osteoporosis, are also a source of back pain.
The precise mechanism explaining back pain involves nociceptive stimulation of pain receptors located throughout the spine, particularly in the intervertebral discs. These receptors, stimulated by any kind of injury or degenerative condition, transmit their information to the brain, which interprets it as pain.
Risk factors
- Accidents involving the back, sometimes even of low intensity, especially if they occur repeatedly.
- Some sports activities are too intense, especially if carried out without adequate preparation.
- Repetitive axial (vertical) stresses, performed too intensely (jogging on hard surfaces, ski jumping, lifting weights, etc.). Poor back hygiene, especially at work, and poor sitting postures.
- Being overweight.
- Poor physical condition and in particular a lack of muscle structure, often linked to age.
- Sedentary professions.
- Anterior disc surgery.
- Back fractures.
- Osteoporosis
Screening & Diagnosis
Because the causes of back pain are numerous and varied, it's understandable that diagnosis isn't always straightforward. A doctor's examination can help differentiate between simple lower back pain and more complex cases. Depending on the circumstances, the medical examination may need to be supplemented with radiological investigations (X-rays, CT scans, MRIs, etc.) to better understand the problem. These tests will be prescribed by your doctor in cases of chronic or recurring back pain, especially if conservative treatment has been ineffective.
In rare cases that are particularly complicated and resistant to treatment, the specialist physician may be led to perform more complicated examinations, sometimes carried out in pain management centers, such as discography, facet joint blocks or intradural injections.
Treatments
Self-treatment
Most back pain not related to a serious structural cause will gradually decrease and disappear spontaneously within a few days. The patient can then undertake a simple treatment that will facilitate or even accelerate recovery.
- Decreased physical activity
- Rest
- Lying down, with a cushion under your knees
- Over-the-counter pain relievers and anti-inflammatory medications. Massages
- Heat (heating pad, hot bath, hot shower, etc.)
- Anti-inflammatory patch
- Heating ointment or balm
Medical treatments
Patients with particularly severe or persistent back pain should consult their doctor. Management of lower back pain will always begin with a well-directed conservative treatment plan, including a reduction in physical activity (with a few days of rest if necessary), combined with pain-relieving medication, pain-relieving physiotherapy, abdominal strengthening exercises, and possibly osteopathy.
Especially in cases where lower back pain is caused by degenerative processes and osteoarthritis, conservative treatment can be extended with infiltrations, mainly facet joints.
Surgical treatment may be considered when the pain is particularly severe and persistent despite conservative treatment for at least 2 to 3 months.
Our favorite methods
Conservative treatment
At our back center, we begin by optimizing non-surgical treatment. In addition to medication, we place particular emphasis on an aggressive physiotherapy approach. The program will focus on muscle relaxation techniques, spinal mobilization, and, most importantly, strengthening the muscles that stabilize the back. These measures will be combined, whenever possible, with a program performed both on land and in a pool, as water is particularly effective in promoting patient relaxation.
Epidural and facet joint infiltrations
To maximize treatment and enhance the anti-inflammatory effect, epidural or facet joint injections are sometimes recommended, especially when the patient is experiencing degenerative changes and osteoarthritis in the lower back. These procedures are performed under local anesthesia. Under radiological guidance, a needle is inserted into the spinal canal (into the epidural space) or into the posterior facet joints, where small amounts of cortisone are injected to provide maximum anti-inflammatory relief. These injections are performed on an outpatient basis, and the patient can return home after a one-hour follow-up at the clinic. If the patient's symptoms improve, these injections can be repeated at intervals determined by the physician (3 to 6 weeks).
Surgical management
If lower back pain persists and is debilitating despite appropriate conservative treatment for at least two to three months, surgical treatment may be considered. In some particularly complex cases, selection for surgery will require further investigations (discography, specific injections) performed at our pain management and back pain diagnostic center to better identify the exact cause of the lower back pain. When lower back pain is caused by discopathy (severe disc degeneration, severe tear of the annulus fibrosus, following surgery for a herniated disc, etc.), the surgeon will need to perform a radical resection of the diseased disc combined with spinal fusion (spondylodesis) or the placement of an artificial disc (disc prosthesis).
Spinal fusion
Spinal fusion (spondylodesis) procedures are performed under general anesthesia via a posterior approach, through an incision of approximately 10 cm in your lower back. The exact location of the skin incision is determined radiologically before the procedure begins. The muscles covering the spine are then separated to allow the surgeon access to the posterior part of the spine, opening the spinal canal that carries the nerves and thus accessing the diseased intervertebral disc. Using a posterior approach and guided by an operating microscope, the entire disc structure is progressively removed with microsurgical instruments. The removed disc structure is then replaced with small cages, the same height as a normal disc, pre-filled with bone. These cages will provide axial support between the two vertebrae on one side and support for the bone graft (fusion) that will take place in the following months on the other. To provide immediate stability, spinal fixation (instrumentation) is used, allowing for rapid patient mobilization after surgery and offering optimal conditions for bone graft consolidation. These spinal fixations are achieved using titanium screws and rods. Implant placement is performed using computer-assisted navigation, ensuring ideal implant positioning and minimizing the risk of malposition.
Disc prosthesis
In certain selected cases (young patients with disc pathology without compression of nerve structures and without degenerative pathology of the posterior facet joints), the placement of an artificial disc (disc prosthesis) may be considered. This surgical procedure is performed via an anterior approach. It is a delicate operation, involving a 6- to 7-cm incision in the suprapubic region. The surgeon must first reposition the abdominal viscera and the major blood vessels (aorta and vena cava) to access the anterior aspect of the spine. Through this access, the diseased disc is radically resected and replaced with a disc prosthesis. The precise positioning of the implant is performed under fluoroscopic guidance to ensure it is perfectly centered in the intervertebral space created by the disc resection. The disc prosthesis is an implant consisting of a plate that can move in all directions on a spherical surface; it generally consists of two parts coupling a metal plate with a polyethylene part (extremely strong plastic) and allows a movement of about 5° in all directions, which is close to the natural mobility of the disc.
After the operation
Upon leaving the operating room (you will be awake and lying on your back), you will be transferred to the recovery room where you will stay overnight to ensure optimal monitoring and care. Visitors are generally allowed in the recovery room (approximately one hour after your discharge from the operating room, limited to one person at a time).
In the recovery room, you will be under the care of the anesthesia team, who will monitor you and administer pain medication. Every effort will be made to ensure your comfort and keep your pain under control. A urinary catheter may be inserted in the operating room (operation duration: 2 hours, for elderly patients).
It will be left in place for one to two days to avoid the discomfort of the vase, and is usually removed when you are able to use the toilet yourself. At the end of the procedure, the surgeon will insert a drain into the surgical wound to remove post-operative bleeding. This will be removed by your surgeon, usually 48 hours after the procedure.
To reduce the risk of thromboembolism (the formation of blood clots in the veins of the lower limbs and in the lungs), the patient will need to wear compression stockings on both legs for a few days. Subcutaneous injections of an anticoagulant will be administered every evening until discharge from the clinic.

Surgery
Preparation for surgery
We will be in constant communication with your family doctor to discuss and proceed with the best treatment option for you. Once the surgical indication has been determined and scheduled, you will receive a summons letter from the Bois-Cerf Clinic containing information regarding:
Pre-hospitalization consultation
Before your hospital stay, you will have a consultation with one of our anesthesiologists to assess your health, perform the necessary tests (blood work, chest X-ray, electrocardiogram), and discuss the anesthesia procedure, which will be general anesthesia. Please be informed of the day and time you should arrive at the reception desk of the Bois-Cerf Clinic (this could be the day before or the day of the procedure).
Hospital stay
What you need to bring with you:
- Your personal belongings
- Reading material if you enjoy reading
- Music player
- Your personal medications (if you are receiving treatment at home)
- Your optimism and energy. We'll take care of the rest.
Upon your arrival at the clinic, after completing the administrative formalities, you will be greeted by the receptionists and shown to your room. The nursing staff will take care of you to ensure you are comfortable. Some tests may still be necessary as requested by your doctors. Skin care (disinfection) will be performed on the area of the future surgical wound.
You will receive visits from your surgeon and the anesthesiologist (pre-operative visits). A physiotherapist will visit to instruct you on breathing exercises and how to move in bed and get up after the procedure. The surgery will generally be performed at the time previously communicated to you by your surgeon.
As in the past, the operation is performed under general anesthesia. Your anesthesiologist will administer premedication one hour before the operation and, if necessary, the evening before, to help you relax and reduce stress related to the procedure. Visitors are generally allowed in the recovery room (approximately one hour after you leave the operating room, one person only) and freely in your hospital room.
Recovery
The patient will be up and mobilized from the day of the operation or the following day, under the supervision of his physiotherapist or nursing staff.
The urinary catheter, surgical drain, and intravenous line will generally remain in place for 48 hours to better manage postoperative pain and allow the patient sufficient time to get up independently and use the toilet. A shower is permitted on the third or fourth postoperative day.
During hospitalization, physiotherapists will teach the patient rehabilitation exercises and how to properly perform daily living activities. Wearing an elastic lumbar support brace is recommended for 2 to 3 weeks after disc replacement and for 6 weeks after spinal fusion. Hospitalization is usually 5-6 days for disc replacements and 10-12 days for fusions, and also depends on the patient's progress and situation at home.
Post-operative pain is relieved during the first few days via an intravenous line connected to a pain pump that the patient can adjust themselves. Subsequently, pain medication will be prescribed to ensure adequate pain relief, depending on the patient's level of physical activity. Sutures or staples from the surgical wound are removed 10-12 days after the procedure.
Some discomfort and back pain are always present after the operation and will gradually decrease as the muscles heal. Once you return home, you should lead a quiet life (you are in recovery). You will need to pay attention to the surgical wound (according to the instructions received during your hospital stay). For the first 2 to 3 weeks, you should avoid sitting in low positions (sofa, armchair), avoid strenuous physical activity (household chores), and avoid lifting/carrying heavy objects.
A clinical check-up is scheduled approximately 4 to 6 weeks after the procedure to plan the follow-up (medication, physiotherapy, resumption of activity, sick leave, etc.).
Rehabilitation
A physiotherapy rehabilitation program will begin after the initial medical visit. Physiotherapy focuses on restoring muscle function and strengthening the abdominal muscles, flexibility exercises (neuromeningeal stretching), and progressive mobilization of the lumbopelvic junction. This program may be conducted on land, sometimes with the assistance of a swimming pool. The recovery rate varies from patient to patient and usually requires 4 to 8 weeks off work for prostheses and 3 to 4 months for fusions. Driving will be possible as soon as you can sit comfortably and without pain, generally 3 to 6 weeks after the procedure. Approximately 80% of patients experience good relief from their lower back pain with this type of surgery.
Frequently Asked Questions
How long does the operation take?
Where is the scar?
What is the length of the incision?
Is the operation possible by numbing only the legs (epidural anesthesia)?
When I leave the operating room, will I be lying on my stomach?
How many days will I stay in the clinic?
Will I be in a lot of pain after the operation?
When can I start driving my car again?
What mobility will my back have after a spinal fracture?
When can I return to work?
After an epidural injection, when can one resume physical activity?
Should we be concerned about the use of cortisone during epidural infiltration?
Summary
1006 Lausanne
+41215103348
Learn more in videos
Medicol Videos

28:22

16:03
Contact one of our specialists on the subject
Ouchy Orthopedic Center
Specialized medical consultations in orthopedics and traumatology in the heart of Lausanne