














- Welcome
- Ligament injuries
Ligament injuries
##Anatomical_zone##
Introduction
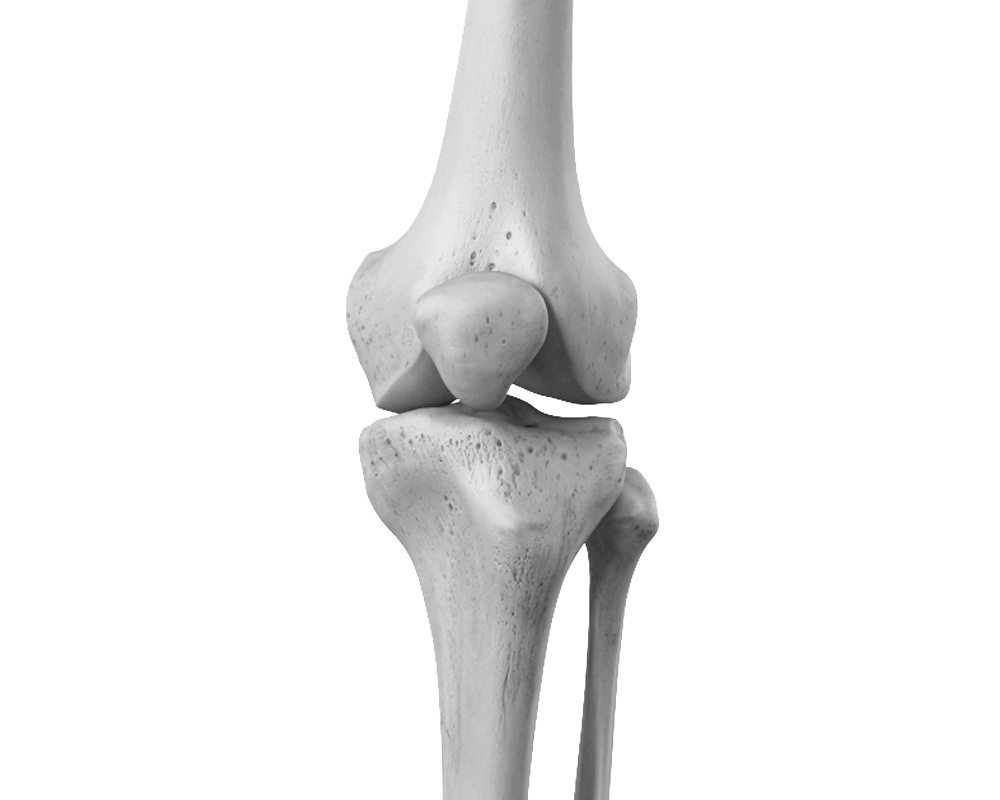
The knee comprises two distinct joints: a weight-bearing condylar joint formed by the femur and tibia, divided into two compartments, medial and lateral, and a trochlear joint formed by the patella and femur. The patella is a sesamoid bone, meaning a bone embedded within a tendon (in this case, the quadriceps tendon). This joint guides the knee's extensor mechanism and amplifies the force of the quadriceps muscle located on the anterior aspect of the thigh.

Do you need the advice of a specialist?
Consult a doctor at the Ouchy Orthopedic Centre.

Anatomy
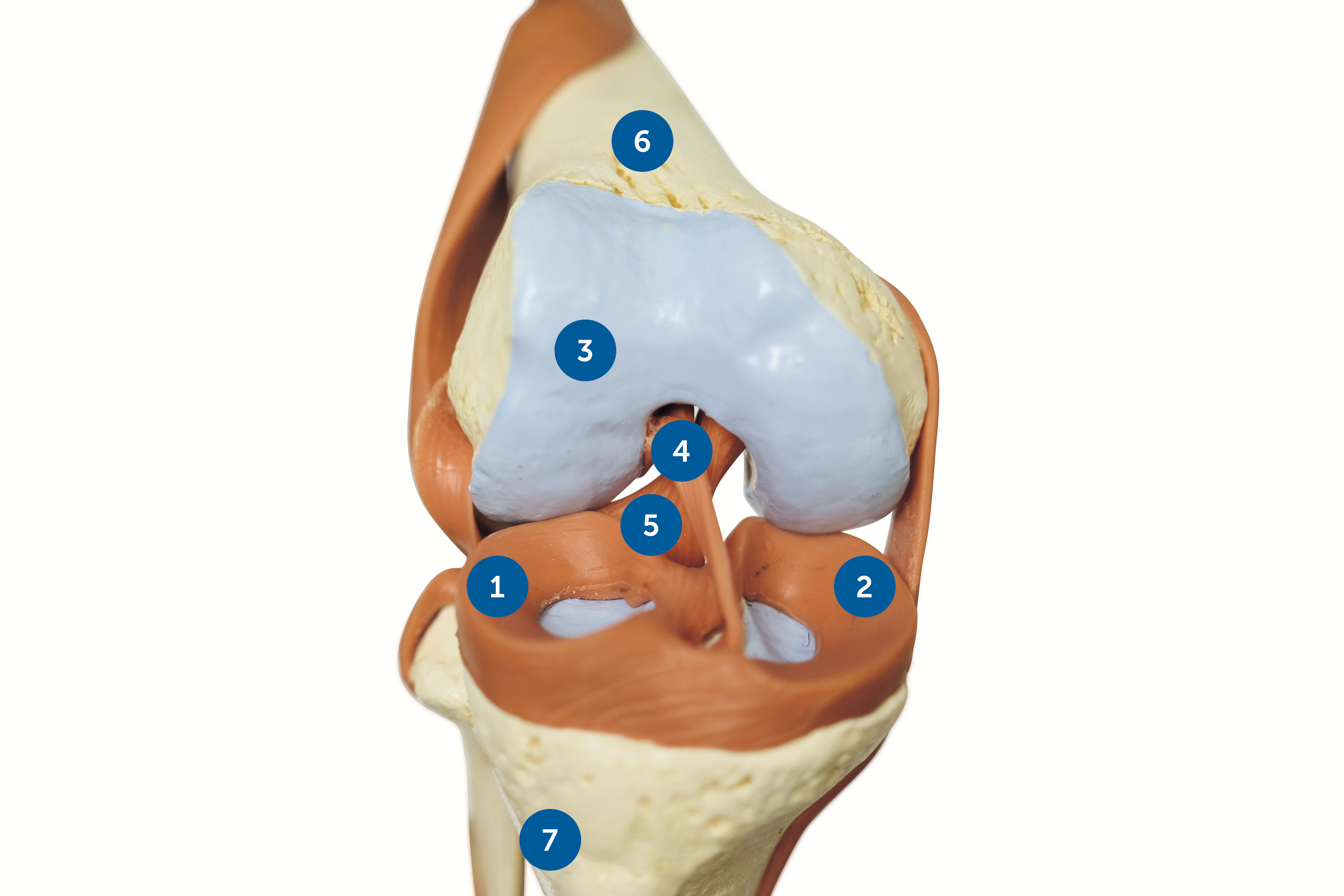
External meniscus (1), Internal meniscus (2), Cartilage (3), ACL (anterior cruciate ligament) (4), PCL (posterior cruciate ligament) (5), Femur (6), Tibia (7).
The knee comprises two distinct joints: a weight-bearing condylar joint formed by the femur and tibia, divided into two compartments, medial and lateral, and a trochlear joint formed by the patella and femur. The patella is a sesamoid bone, meaning a bone embedded within a tendon (in this case, the quadriceps tendon). This joint guides the knee's extensor mechanism and amplifies the force of the quadriceps muscle located on the anterior aspect of the thigh.
Inside the joint, the bones are covered with cartilage, a very smooth and flexible tissue that facilitates the gliding of the articular surfaces against each other and simultaneously cushions impacts. The ligamentous apparatus of the knee stabilizes the joint and controls joint movement; it is composed of the cruciate ligaments in the center of the joint and the collateral ligaments on the periphery.
The menisci are made of fibrocartilage. Attached to the capsule but nonetheless mobile, their role is to stabilize, shock-absorb, and also lubricate the cartilaginous surfaces. The medial meniscus has a crescent shape, while the lateral meniscus, which is thicker, has a more disc-like appearance.
Signs & symptoms
An anterior cruciate ligament (ACL) tear occurs primarily during sports activities such as football, skiing, and basketball. The injury usually happens during a sudden change of direction or when landing from a jump while losing balance.
Symptoms of an anterior cruciate ligament (ACL) tear include: a popping sound in the knee at the time of injury, a feeling of the knee giving way, the need to stop activity due to pain, and the inability to fully bend or straighten the knee. In the hours that follow, swelling of the knee frequently appears, indicating bleeding within the joint.
Mechanism of tearing
ACL injuries account for between 100,000 and 200,000 cases per year in the USA, according to a recent study published in 2020 by Harvard University. Sprains occur during non-contact trauma in sports activities involving pivoting movements, such as ball sports, sliding sports, combat sports, or gymnastics. A sprain occurs during a sudden deceleration combined with a change of direction that unbalances the knee, or upon landing from a jump followed by a valgus collapse of the knee. This sudden movement is due to a pronated foot roll that causes the knee to spiral into a valgus-internal tibial rotation, a phenomenon known as medial collapse of the knee.
Other mechanisms exist, notably direct impacts, but these are much less frequent. Associated injuries, especially meniscal tears, are present in about half of cases and are treated simultaneously during surgery.
Risk factors
- Functional hallux limitus (learn more This induces a sudden pronated translation at the end of the stance phase, which causes the knee to rotate, resulting in significant stress on the ACL.
- Activities such as ball sports, where sudden changes of direction are frequent, make the ligament more susceptible to injury. In skiing, the foot and ankle are immobilized, and the knee, particularly the anterior cruciate ligament, must bear additional stress.
- Poor physical condition and muscle fatigue predispose individuals to sprains. An unpredictable movement at the end of a game or the end of the day can have more serious consequences for the knee.
- Lack of balance and coordination: when walking on uneven ground, for example, instability of the ankle and foot induces compensatory mechanisms that expose the knee to ligament damage.
- Each individual's unique anatomical makeup can predispose them to anterior cruciate ligament injuries, such as legs shaped like "parentheses", excessive lumbar curvature, etc.
Screening & Diagnosis
Clinical examination is sufficient in almost all cases to diagnose an anterior cruciate ligament (ACL) injury. This examination is sometimes difficult in emergency situations due to pain and muscle spasms around the knee. The presence of blood in the joint after a knee sprain indicates an ACL tear in more than 70% of cases.
Two clinical maneuvers are specific for diagnosing an anterior cruciate ligament injury: the anterior drawer test at 20° of flexion called the Lachman test, and the tibial pivot shift maneuver in front of the femur called the pivot shift or Losee test.
X-rays of the knee are generally normal. Magnetic resonance imaging (MRI) demonstrates the anterior cruciate ligament (ACL) tear and also allows for the diagnosis of associated injuries, particularly meniscal or osteochondral lesions. These lesions are present in more than half of ACL tears.

Treatments
Self-treatment
If you have experienced a severe knee sprain with the symptoms described above, you should consult an orthopedic surgeon before resuming your sporting activities. In the presence of instability, secondary meniscal tears and premature wear of the articular cartilage are sometimes observed. Repeated episodes of instability generally indicate the need for surgical reconstruction of the anterior cruciate ligament (ACL).
Medical treatment
An anterior cruciate ligament (ACL) injury can lead to significant blood effusion in the knee, thus putting the joint under stress; in this case, early aspiration is recommended. Locally, inflammation and pain should be managed by reducing weight-bearing on the knee according to the pain level (using crutches) and applying ice 5 to 6 times a day to relieve pain. If the ACL injury is isolated, immobilizing the knee in a brace is not necessary.
It is important not to leave the patient to their own devices and to offer physiotherapy promptly in order to prevent muscle atrophy and loss of knee joint control. Physiotherapy includes local treatment with lymphatic drainage massage, active knee stabilization and muscle strengthening exercises, as well as gait retraining.
Surgical treatment
Unfortunately, cruciate ligament repair by suture or bone reattachment is only possible in a very small percentage of cases. Most often, the tear is located deep within the ligament, and a simple suture is insufficient to guarantee knee stability. Ligament reconstruction is therefore necessary, and several techniques exist, using different grafts or fixation methods specific to each surgeon. The prognosis after surgical treatment is generally good.
Surgical treatment is indicated in cases of knee instability (repeated buckling, pain when bearing weight, etc.) and depending on the type of activities the patient wishes to resume after their ligament tear. Surgery generally takes place within weeks of the injury, once the knee is stable, the patient has regained mobility, and walking without a limp is possible. Surgical treatment may sometimes be necessary on an emergency or delayed basis in cases of severe multi-ligament injury or fracture. These indications are rare.
The principle of surgical ACL reconstruction involves rebuilding the anterior cruciate ligament with a tendon graft (autograft or allograft) that faithfully reproduces the tension and natural position of the anterior cruciate ligament. The operation is performed under arthroscopic guidance to ensure proper placement of the new ligament.
Our favorite method
The anterior cruciate ligament is reconstructed under arthroscopic guidance using an autologous semitendinosus tendon graft (a single tendon). This tendon is harvested using a stripper and allows for a four-bundle ligament reconstruction with initial strength superior to that of the original anterior cruciate ligament. The graft is fixed to the femur with two absorbable transfixing nails. On the tibia, traction sutures are laced around a small steel pin screw. This screw is usually not a problem but can be removed under local anesthesia if necessary. This technique has been performed successfully for many years, and recent studies highlight its excellent results.David P Trofa, Am J Sports Med 2020The crucial point is the correct positioning of the graft. This technique results in fewer complications on the extensor mechanism than using a patellar tendon graft and also has cosmetic advantages.
Surgery
Preparation for surgery
Your family doctor's involvement
Once the indication for surgery has been established, your doctor can, depending on the needs, arrange the necessary tests to complete the pre-operative assessment by the anesthesiologist.
You will receive a summons letter from the Clinic with information regarding:
Pre-anesthesia consultation
Before surgery, you will be seen by one of our anesthesiologists who will ask you about your medical history before conducting a clinical examination. You will then be able to discuss the different methods available and choose the most suitable one for your specific case (general anesthesia, spinal anesthesia, nerve blocks, combined anesthesia).
Surgery
What you need to bring with you:
- Your personal belongings
- Reading material if you enjoy reading
- Music player
- Your personal medications (if you are receiving treatment at home)
- Your optimism and energy... we'll take care of the rest.
Post-operative pain management
The anesthetic strategy will be specifically designed according to your health, your wishes, and the type of surgical procedure, with the aim of guaranteeing you will experience no pain upon waking and during rehabilitation. There are multiple effective solutions available.
Recovery
Rehabilitation following anterior cruciate ligament reconstruction is designed to respect the biological principles of tendon graft healing and the healing of associated injuries. Gait retraining begins on the day of surgery, initially with partial weight-bearing (half body weight) and then gradually with full weight-bearing. Each individual's progress is unique and should be respected as much as possible. The program is generally divided into three phases before resuming training.
Phase 1: Weeks 1 and 2:
To recover a calm and pain-free knee, maintain muscle trophicity in the thigh and physical condition, regain active control of the knee, control balance through a good feeling of support on the ground, control pelvic stability and regain a harmonious gait, plan progression and set goals to achieve.
Phase 2: Weeks 3, 4 and 5:
Regain a limp-free gait with full weight-bearing, regain knee mobility, particularly active full extension. Improve active knee control in situations of imbalance, resume cycling, step aerobics, and certain swimming activities.
Phase 3: from the 6th to the 12th week:
Secure footing and train movements, strengthen muscles in jumping school, improve fluidity of movement, train coordination, symmetrize and synchronize walking and running, regain full mobility
The knee's reaction (pain or swelling) must be taken into account in the progression margin, inflammation and sudden movements should be avoided, and a steady progression should be aimed for.
During the stay in the clinic
On the day of the procedure, from the recovery room:
Feel the contraction of the calf and thigh muscles, perform circular movements with the ankle and mobilize the hip and knee below the pain threshold.
Day 1 post-operative:
Continued pain medication and infusions, removal of the drain, regular application of ice, recovery of active control of the lower limbs, active and passive mobilization of the knee, start of gait rehabilitation, co-contraction muscle strengthening exercises.
2nd postoperative day:
Removal of the IV line, continued application of ice and active and passive mobilization of the knee, gait retraining, patellar mobilization and massage-drainage. First shower possible.
3rd postoperative day:
Continuation of the various treatments undertaken, with emphasis on regaining independence in walking, including on stairs, and learning the different exercises to do at home; gait rehabilitation aimed at regaining the best possible active control of the knee and a good sense of balance when in contact with the ground; intensification of muscle strengthening exercises.
Return home
To best prepare for your return, you should have several certificates, prescriptions, and information, including: anti-inflammatory, pain-relieving, and anti-thrombotic medication; a physiotherapy prescription (sessions should be taken 2 to 3 times per week); an appointment with your surgeon for dressing changes, suture removal, and a clinical check-up; and a detailed rehabilitation program.
At home, the exercises should be performed at least twice a day in sessions lasting approximately one hour, with all exercises grouped together. It is important to allow for recovery time. The intensity of the exercises should be adjusted according to knee swelling and pain. It is essential to walk at least twice a day for half an hour each time with crutches, avoiding a limp.
Possible risks
The infection
Infection is always a serious complication in orthopedic surgery, but fortunately very rare (less than 0.51 TP3T). Specific measures are taken to minimize these risks, including: systematic pre- and immediate post-operative antibiotic therapy, operating rooms equipped with high-flow laminar airflow, a highly trained and experienced orthopedic surgical team, optimal skin preparation, and a careful assessment of your health.
If you experience fever or local redness after your procedure once you have returned home, you must call your surgeon immediately.
Venous thrombosis and pulmonary embolism
Venous thrombosis is characterized by the blockage of a vein by a clot (thrombus), which prevents blood from returning to the heart. If the clot migrates, it can in turn obstruct the pulmonary vessels, resulting in a pulmonary embolism. To minimize these risks, a tourniquet is not used during your procedure; prophylaxis is administered through subcutaneous injections of low molecular weight heparin, and gait rehabilitation begins as soon as possible.
Thromboembolic prophylaxis will be prescribed for 5 to 10 days from your intervention in the form of a daily subcutaneous injection of Clexane 40 mg or Xarelto 10 mg tablets.
If you experience calf pain or a tight appearance of the calf during the postoperative phase at home, you must call your surgeon immediately.
Nerve damage
It is possible that you may experience decreased sensation on the outer side of your proximal tibia after surgery, due to stretching of a superficial nerve branch. The incision is made near a sensory branch, which can be stretched during the procedure. Sensation usually returns after several weeks.
Bleeding
Generally, the procedure does not cause significant bleeding because the access point is very small and the procedure is performed arthroscopically. In cases of significant joint effusion, aspiration is sometimes necessary.
Functional limitation:
In a small percentage of cases, the knee does not regain its full range of motion. This can be due to muscle weakness, the formation of scar tissue, or adhesions within the knee. Proper graft placement and effective, personalized rehabilitation minimize this risk, but the cause is not always clear. Treatment for these delayed recoverys is now better standardized.
Residual instability
Depending on the morphology of the lower limbs or associated injuries, ACL reconstruction may be complemented by other surgical procedures. The rehabilitation program should then be adapted to prevent recurrence of instability.
Frequently Asked Questions
What kind of scar will I have?
What sports will I be able to do after my procedure?
How long will I need to wear a splint?
How long will I need to use crutches?
How long does the healing process take to integrate the new ligament?
When will I be able to take a shower?
When will I be able to drive?
Summary
1006 Lausanne
+41215103348
Learn more in videos
Medicol Videos

17:46

16:25

26:04

12:00

15:00

17:07

16:28
1:19:31
Contact one of our specialists on the subject
Ouchy Orthopedic Center
Specialized medical consultations in orthopedics and traumatology in the heart of Lausanne