














- Welcome
- Hallux valgus
Hallux valgus
Foot
Introduction

Anatomy
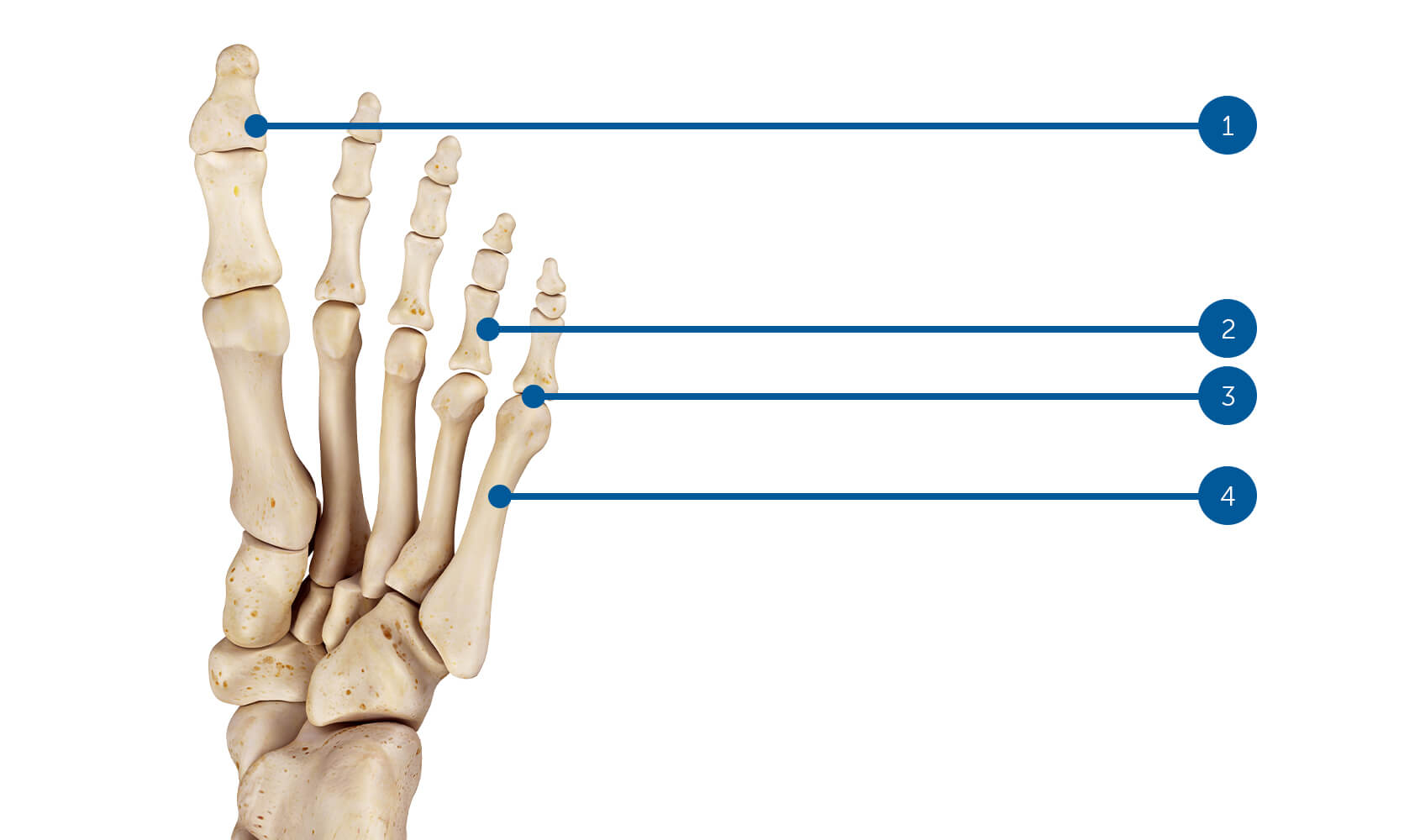
(1) Distal phalanx, (2) Proximal phalanx, (3) Metatarsophalangeal joint, (4) Metatarsus.
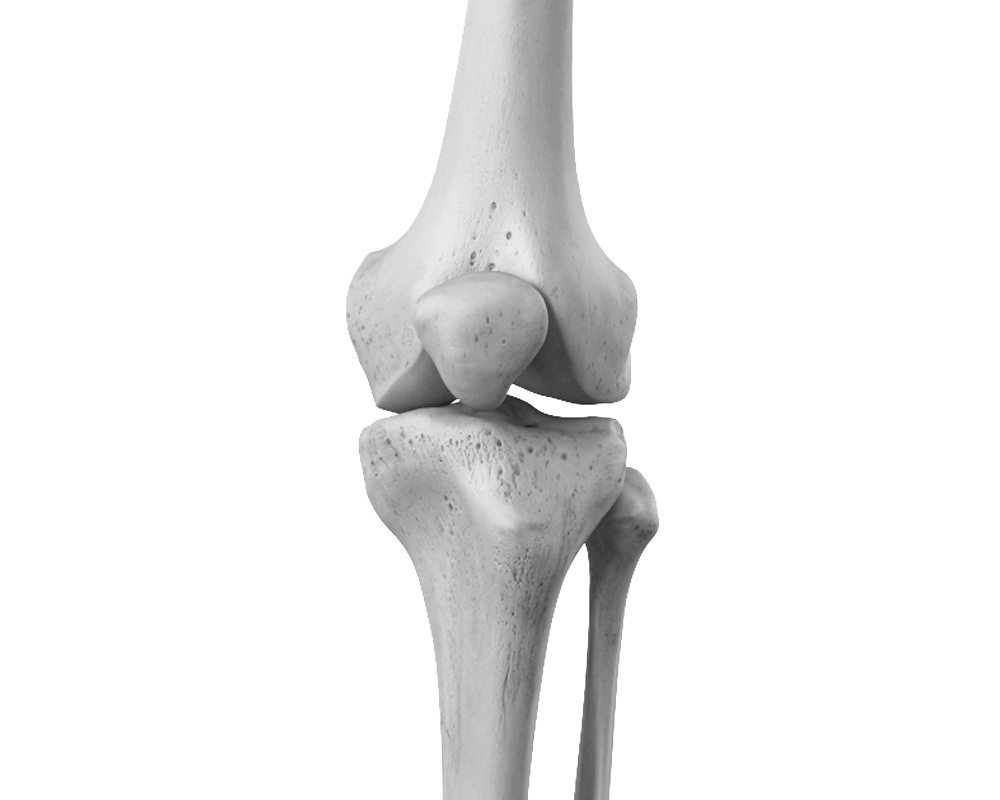
The ankle is a hinge joint, and the talus is held in a mortise-like position between the two malleoli. Below, the talus articulates with the calcaneus, and anteriorly with the navicular bone, forming the subtalar joint with the cuboid bone. This joint was called the "coxa pedis" by Pisani because of its similarities to the hip joint. Its stabilizing action allows us to walk on uneven ground while maintaining our balance on one foot. Furthermore, it synchronizes gait by facilitating the transition from pronation to supination or vice versa.
The midfoot is composed of the tarsometatarsal joints between the 3 cuneiforms, the cuboid and the metatarsals.
The forefoot is formed by the metatarsophalangeal joints and the interphalangeal joints of the toes. The forefoot is connected to the hindfoot by a complex network of tendons, ligaments, and small muscles, and this system constitutes a powerful dynamic lever in the transmission of forces during walking.
Signs & symptoms
Deformation:
The forefoot widens and flattens, and a bony protrusion appears on the inner edge of the first metatarsophalangeal joint. This bony growth, called a bunion, rubs against the shoe, causing pain from pressure and irritation. Additional pain may occur at the heads of the second and third metatarsals, resulting from a transfer of weight-bearing from the first metatarsal to the midfoot.
Calluses:
Calluses appear particularly on the inner side of the first toe, as propulsion no longer occurs along the axis of the big toe but on its edge.
Imbalance:
The deformity alters propulsion, which can no longer be exerted on the ball of the big toe. Functionally, the foot is shortened and deprived of an important stabilizing lever. Balance is thus compromised.
What is this?
Hallux valgus results from a dislocation on the medial side of the first metatarsophalangeal joint. The first metatarsal separates from the second, the medial capsule tears, and the toe, remaining connected to the plantar and lateral capsuloligamentous structures, is deviated onto the second ray. A collapse of the forefoot is always present, often associated with a claw-like retraction of the toes.
Risk factors
Various causes are cited as predisposing factors to deformity: family predisposition, high heels, shoes that are too narrow, Greek or Egyptian foot shape, being overweight, etc.
Functional Hallux Limitus or Functional Hallux Rigidus, described in another chapter of this site, is, in our opinion, one of the main causes of hallux valgus deformity. This condition manifests as a lack of freedom of movement in the tendon of the flexor hallucis longus, which then, through a rope-like effect, induces significant tension on the first metatarsophalangeal joint, leading to progressive deformity.
Considering this factor as predisposing, we always associate a tendon pulley release procedure of the flexor hallucis longus in surgical corrections of hallux valgus.
Screening & Diagnosis
The assessment of the deformity is clinical: note any excessive pressure points, measure the angle of the deformity, and examine the entire foot. The rotational component of the deformity is also important because the toe frequently turns in opposition to the second toe.
Footprint is studied on a podoscope or on a treadmill.
Radiological assessment is essential before considering surgical correction. This assessment includes an anteroposterior and lateral view, both taken with the foot weight-bearing, an oblique view of the foot, and in some cases an axial view of the forefoot (sesamoid bone view).
Other tests such as magnetic resonance imaging or CT scans are only requested in exceptional circumstances.
Treatments
Self-treatment
Several orthotics are available to passively correct the deformity, but most are ineffective. Plantar supports can help distribute the load more evenly on the forefoot and relieve pain from excessive pressure. Custom shoe fitting, performed by a shoemaker or orthotist specializing in orthotics, to adjust the shoe size at the point of deformity prevents excessive friction, especially in new shoes. Proper rearfoot support improves balance and the natural gait. The use of flip-flops should be avoided.
Medical treatments
Physiotherapy, orthotics, and appropriate footwear can help manage the deformity, alleviate pain, and improve balance while making walking easier. However, once established, the deformity is irreversible.
Surgical treatment depends on functional demand, pain, shape and degree of deformity.
When the deformity is proven and symptomatic, surgical treatment is proposed in the form of bone realignment of the 1st metatarsal associated with recentering of the sesamoid sling by releasing the external structures and reconstitution of the capsule on the medial side of the 1st metatarsophalangeal joint.
Our favorite methods
In cases of early-stage hallux valgus deformity, particularly in juvenile cases, a combined conservative and surgical treatment may be recommended. This treatment may involve endoscopic tenolysis of the flexor hallucis longus muscle and physiotherapy focused on proprioception, foot strengthening, sesamoid bone alignment, and stretching exercises for the soleus and flexor hallucis longus muscles. These measures may be combined with a prescription for orthotics, especially for leisure or sports activities. Proper footwear is crucial, and advice should be sought from a podiatrist. Flip-flops are not recommended.
When a deformity is confirmed and symptomatic, surgical treatment is recommended, consisting of bone realignment of the first metatarsal combined with recentering of the sesamoid ligament by releasing external structures and reconstructing the capsule on the medial aspect of the first metatarsophalangeal joint. Correction of the basal phalanx of the big toe may be added to the bone correction of the first metatarsal. Correction of the deformity of the other toes should be addressed during the same surgical procedure. Endoscopic tenolysis of the flexor hallucis longus is routinely performed. This procedure aims to prevent joint stiffness in the first metatarsophalangeal joint and to limit the risk of recurrence of the deformity.

Surgery
Preparation for surgery
Your family doctor's involvement
We will be in constant communication with your family doctor to discuss and proceed with the best treatment option for you. Once surgery has been indicated, your doctor will arrange the necessary tests to complete the anesthesiologist's pre-operative assessment.
You will receive a summons letter from the Bois-Cerf Clinic with information regarding:
Pre-anesthesia consultation
Before surgery, you will be seen by one of our anesthesiologists who will ask you about your medical history before conducting a clinical examination. You will then be able to discuss the different methods available and choose the most suitable one for your specific case (general anesthesia, epidural anesthesia, spinal anesthesia, regional venous anesthesia, nerve blocks, combined anesthesia).
– What day and what time should I arrive at the reception of the Bois-Cerf Clinic? It could be the day before or the day of the procedure.
Surgery
What you need to bring with you:
- Your personal belongings
- Reading material if you enjoy reading
- Music player
- Your personal medications (if you are receiving treatment at home)
- Your optimism and energy... we'll take care of the rest.
Post-operative pain management
PAIN AFTER THE OPERATION IS UNACCEPTABLE FOR US.
The night before your surgery and again in the hour before your anesthesia, you will receive premedication (a tablet to help you relax). The anesthetic strategy will be specifically tailored to your health, your preferences, and the type of surgery, with the aim of ensuring you experience no pain upon waking and during your rehabilitation.
Bed rest and ice will be helpful during the first few days. Our team will carefully assess the presence and intensity of your pain with you 24/7 and adjust your treatment accordingly.
Recovery
First postoperative day
After the procedure, it's important not to rush things to avoid the formation of a hematoma, which can cause pain for several days. It's generally recommended to stay in bed for the first day after the procedure, keeping the foot of the bed elevated. This slightly elevated position prevents the hematoma from collecting in the toes and putting them under tension.
Staying in bed doesn't mean remaining immobile; it's important to do vascular exercises by mobilizing the ankles, knees, and hips. Applying ice locally is recommended 5 to 6 times a day for 15 minutes and helps reduce pain and inflammation.
Second postoperative day
Get up wearing shoes with heel support and begin gait rehabilitation, starting on flat ground and gradually progressing to stairs and outdoor walking. When not walking, the preferred position is lying down with the foot of the bed elevated. Use crutches if necessary. Change the dressing.
Third postoperative day:
Intensification of gait rehabilitation, if possible without crutches.
Return home
To best prepare for your return home, you should have several certificates, prescriptions, and information; these include: a 10-day supply of anti-inflammatory, pain-relieving, and anti-thrombotic medication. You will also need an appointment with your surgeon two weeks post-surgery for suture removal and a clinical check-up.
Possible risks
The infection
Infection is always a serious complication in orthopedic surgery, but fortunately very rare (less than 0.51 TP3T). Specific measures are taken to minimize these risks, including: systematic pre- and immediate post-operative antibiotic therapy, operating rooms equipped with high-flow laminar airflow, a highly trained and experienced orthopedic surgical team, optimal skin preparation, and a careful assessment of your health.
If you experience fever or local redness after your procedure once you have returned home, you must call your surgeon immediately.
Venous thrombosis and pulmonary embolism
Venous thrombosis is characterized by the blockage of a vein by a clot (thrombus), which prevents blood from returning to the heart. If the clot migrates, it can in turn obstruct the pulmonary vessels, resulting in a pulmonary embolism. To minimize these risks, prevention involves subcutaneous injections of low molecular weight heparin, and gait rehabilitation begins as early as possible.
Thromboembolic prophylaxis will be prescribed for 10 days from the date of your procedure in the form of one subcutaneous injection per day of Clexane 40.
Frequently Asked Questions
When will I be able to walk normally?
Is this operation painful?
When will I be able to drive?
How long does the operation take?
Can I perform the operation on both feet simultaneously?
At what point should the wires be removed?
Summary
1006 Lausanne
+41215103348
Learn more in videos
Medicol Videos
Contact one of our specialists on the subject
Ouchy Orthopedic Center
Specialized medical consultations in orthopedics and traumatology in the heart of Lausanne